Original paper: Probing the potential of mucus permeability to signify preterm birth risk
What is the first thing that comes to mind when you hear the word mucus? For most people, it’s probably the last time they had a cold. Mucus is not usually something we think about unless there’s a problem. However, it is always there, working behind the scenes to make sure that our bodies function smoothly. Mucus lines the digestive, respiratory, and reproductive systems, covering a surface area of about 400 square meters- about 200 times more area than is covered by skin. In addition to providing lubrication and keeping the underlying tissue hydrated, mucus also plays a key role the human immune system. It serves as a selectively permeable membrane that protects against unwanted pathogens while also helping to support and control the body’s microbiome [1].
Mucus is an example of a hydrogel, which is a three-dimensional polymer network that is able to hold a large amount of water. While hydrogels get their structural integrity from this polymer network, the polymer makes up only a small fraction of the material once they are swollen with water [2]. In mucus, this network is made of biopolymer called mucin.
Researchers in the Ribbeck lab at MIT think that mucus is an underappreciated–and understudied–part of the human body. They have developed techniques for characterizing the mucus hydrogel to better understand how it is able to function as a selective filter. In today’s paper, Kathryn Smith-Dupont and coworkers in the Ribbeck lab investigate cervical mucus and try to understand the relationship between mucus permeability, or its ability to be a selective filter, and the risk of preterm birth.
A birth that occurs before 37 weeks of gestation is considered a preterm birth. This can be associated with negative health outcomes for the baby both in infancy and later in life. Preterm birth is the leading cause of death for children 5 years of age and under, and those who survive can face challenges such as learning disabilities and hearing problems [3]. While the causes of preterm birth can be complex and varied, infection in the fluid surrounding the fetus–which is known to trigger preterm birth–is seen in 25-40% of cases. The infecting bacteria are often the same species that are found in the vagina, suggesting that it traveled through the cervical mucus barrier to infect the sterile uterus.
Smith-Dupont and coworkers look for correlations between mucus permeability and preterm birth risk by comparing the cervical mucus in ovulating non-pregnant women with that in pregnant women. Once the pregnant women give birth, their mucus is characterized as low-risk or high-risk depending on whether they had a preterm birth. The cervical mucus in ovulating non-pregnant women is expected to be at its most permeable to facilitate the passage of sperm, whereas in pregnant women the mucus should be less permeable. Whether a microbe makes it through the mucus barrier can be affected by its size, biochemical interaction with the mucin, or a combination of the two.
First, the researchers look at the permeability of the mucus to 1-micrometer spheres. This is comparable in size to both the mucus mesh and bacteria, and is used to see if the structure of the mucin network is hindering transport through the mucus. Next, they look at the permeability of the mucus to nanometer-size peptides (small bio-molecules). These are much smaller than the mucus mesh, so their ability to pass through the mucus is determined by biochemical interactions with the mucus instead of by its structure. By using these two probe sizes, the researchers hope to identify which mechanism is responsible for any differences in the mucus permeability.
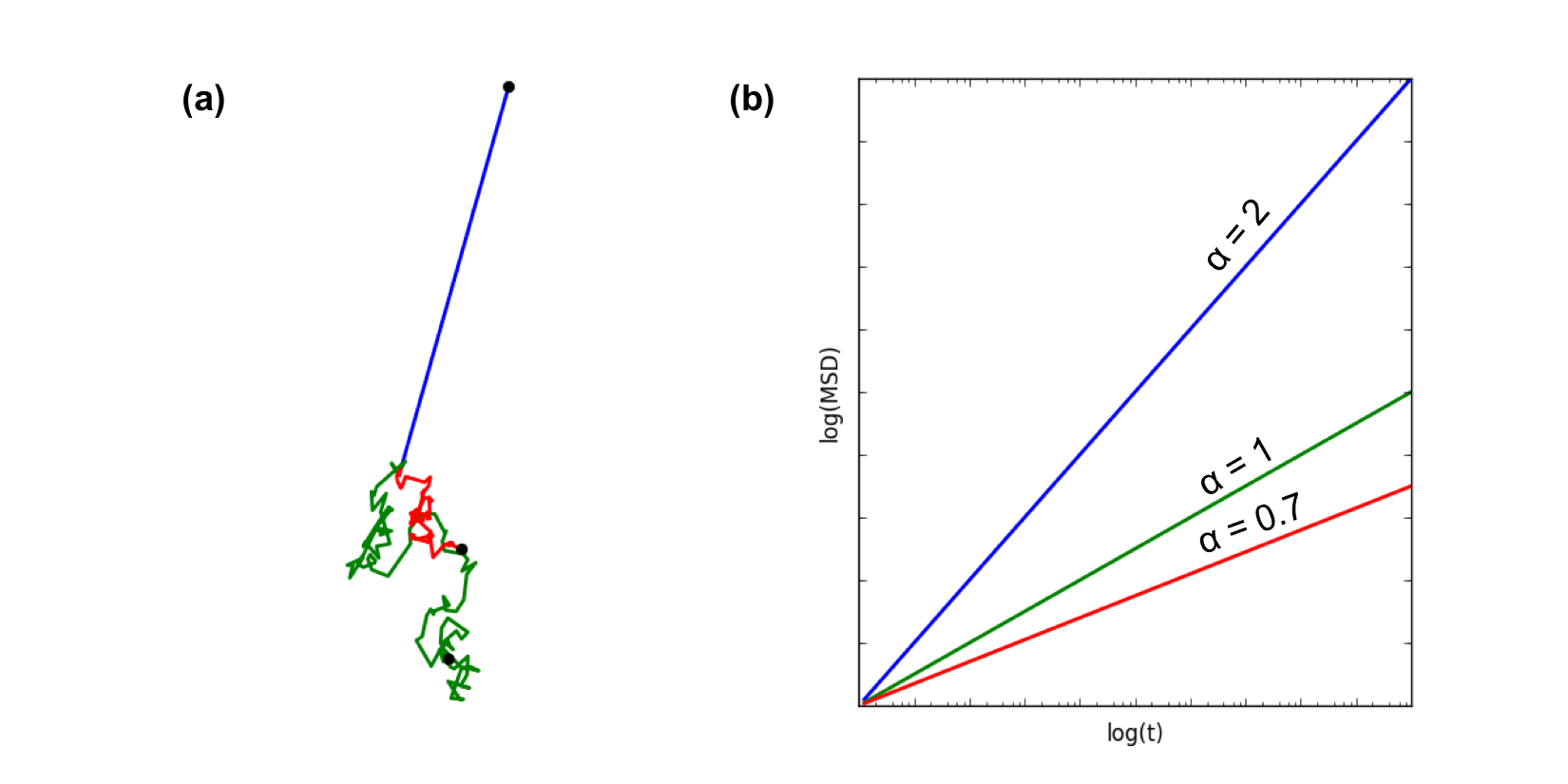
To quantify the motion of 1 micrometer spheres in the mucus, the researchers track the motion of spheres in each mucus sample and calculate their mean square displacement (MSD). A particle’s mean square displacement describes how far it moves, on average, from its starting point in a given amount of time. The MSD is characterized by
$latex \langle r \left( t \right) ^2\rangle = 4 D_{\alpha} t^{\alpha}$
where $latex \langle r^2 \left( t \right) \rangle$ is how far the particle is from its starting point after t seconds and $latex D_{\alpha}$ describes how quickly the particle moves (called the diffusion coefficient). If a particle is acted on by a constant force, it moves in a straight line known as ballistic motion and $latex \alpha = 2$. This is not how a micrometer-scale particle in a fluid moves because it is being bounced around by random forces from the molecules in the fluid. Instead of moving in a straight line, the particle’s trajectory is a series of small excursions in random directions, and it takes longer to get away from its starting point than if it just moved in a straight line. This type of motion is known as free diffusion, and its MSD is characterized by $latex \alpha = 1$. In mucus, the polymer network gets in the way of the particle’s diffusion, so it can’t diffuse freely. This motion is called subdiffusive, and it has $latex \alpha < 1$. The more the particle’s diffusion is hindered by the polymer network, the lower its value of $latex \alpha$ will be. An example of a trajectory and MSD plot for each type of motion is shown in Figure 1.
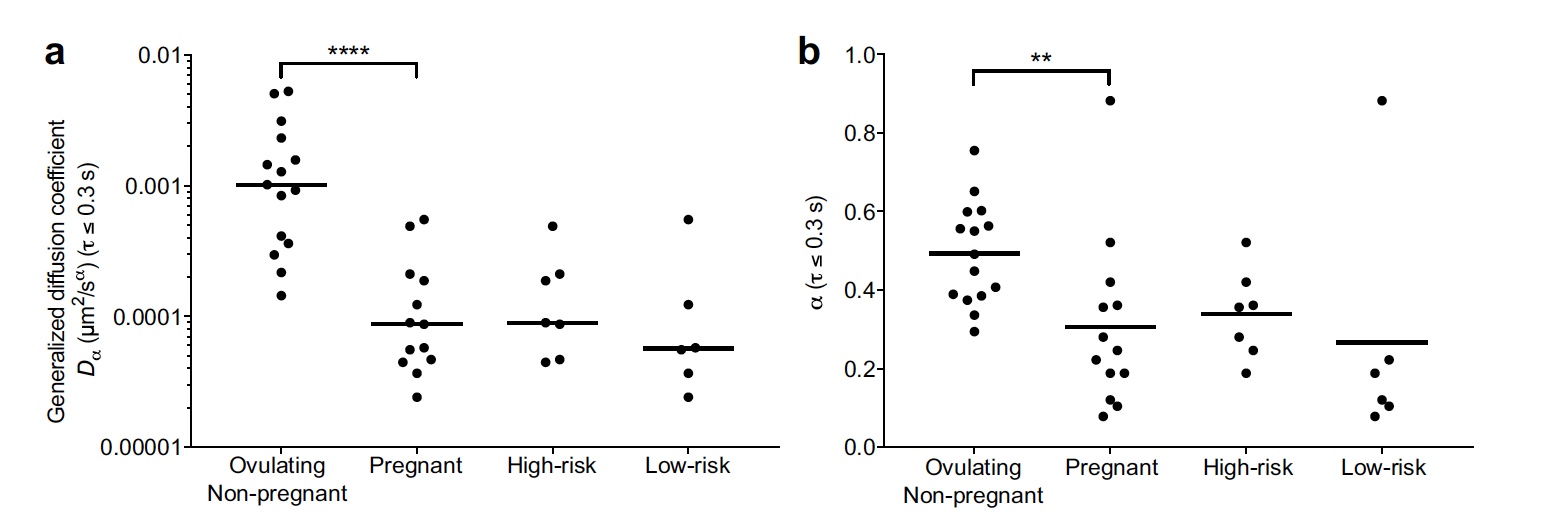
To compare the permeability of the mucus samples, the researchers measure $latex \alpha$ and $latex D_{\alpha}$ for each sample, as shown in Figure 2. The mucus from the pregnant women resulted in lower values of $latex \alpha$ and $latex D_{\alpha}$ than in the non-pregnant women, indicating that the network is more restrictive, as expected. However, the small difference between the high-risk and low-risk pregnancy women was not statistically significant [4]. This suggests that the difference in mucus permeability between high-risk and low-risk pregnancies is not primarily caused by differences in the mucus mesh size.
Next, the researchers look at the permeability of the mucus to small, fluorescently labeled peptides. They use a microfluidic device (to learn more about microfluidics, see [5]) to flow a solution of the peptides through the mucus, and observe whether the peptides get trapped or are able to flow through by looking at the fluorescent profile. Figure 3 shows a schematic of the microfluidic device. The ability of a small particle to travel through mucus is controlled by what happens when it comes in contact with part of the network. This interaction is thought to be affected by the charge of the particle, so the researchers investigate the behavior of both positively and negatively charged peptides.
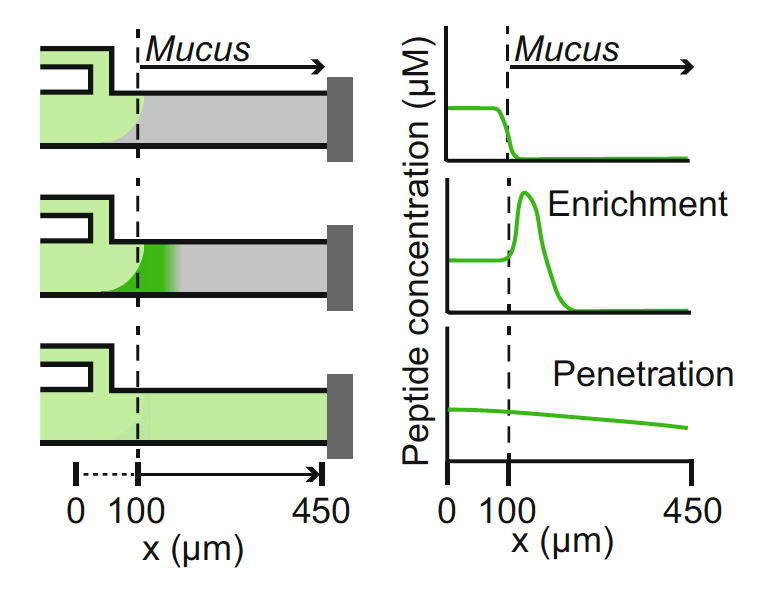
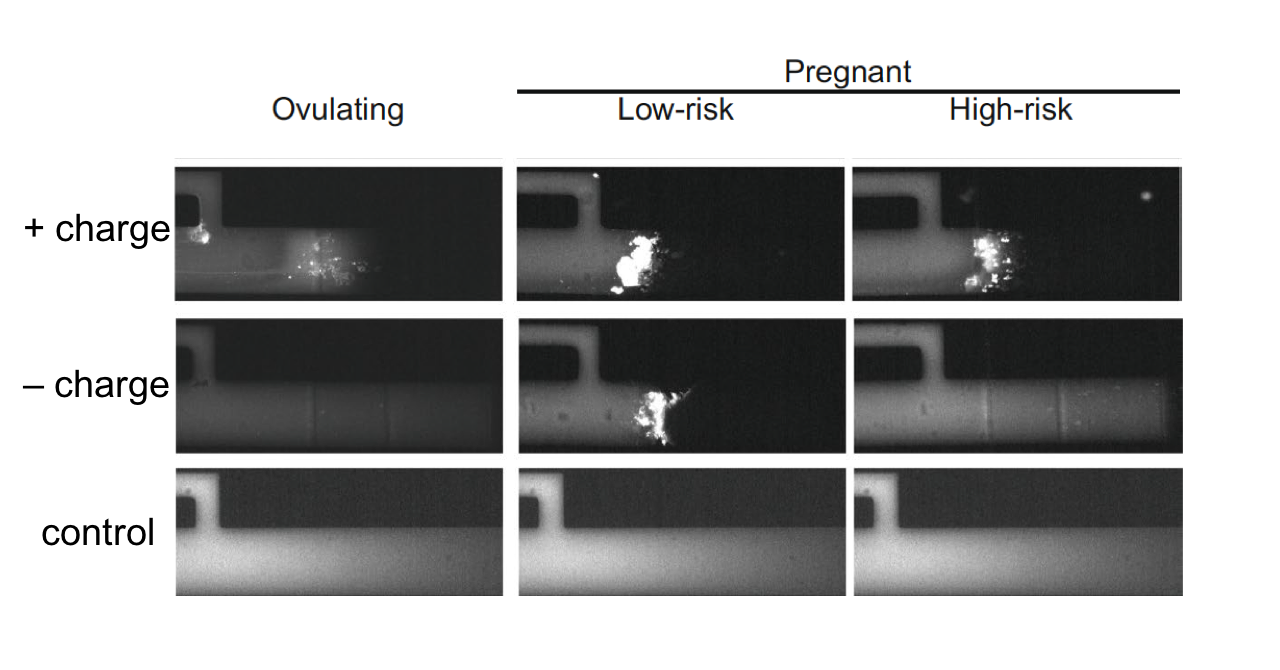
For both positively and negatively charged peptides, the researchers see a significant difference between low-risk and high-risk mucus, as shown in Figure 4. The mucus from both low-risk and high-risk patients was less permeable to the positively charged peptides than the mucus from the ovulating patients. However, more of the positively charged peptides were able to penetrate into the high-risk mucus than the low-risk mucus. The results for the negatively charged peptide were more dramatic. While the low-risk mucus was not permeable to the negatively charged peptide, the high-risk mucus was as permeable as that from the ovulating patients. This suggests that the biochemical properties of the cervical mucus in low-risk and high-risk patients are primarily responsible for differences in permeability.
The results in this study help to clarify which properties of cervical mucus cause an increased risk of preterm birth. The researchers considered both structural and biochemical origins for the increased permeability of cervical mucus to harmful pathogens. Structural changes in the mucin network do not appear to be the primary difference between cervical mucus in low-risk and high-risk pregnancies. Instead, biochemical changes in the mucus that affect how the mucus interacts with microbes appear to be the primary cause of its increased permeability in high-risk pregnancies. This understanding could be useful for developing diagnostic tools to determine a woman’s preterm birth risk and, ideally, treatment to reduce her risk.
[1] https://en.wikipedia.org/wiki/Mucous_membrane#cite_note-Sompayrac-3
[2] Ahmed, Enas M. (2015). Hydrogel: Preparation, characterization, and applications: A review. Journal of Advanced Research, 6(2), 105-121.
[3] http://www.who.int/mediacentre/factsheets/fs363/en/
[4] While the difference between high-risk and low-risk pregnant women is not significantly significant, this does not rule out a difference between the two. The sample size is relatively small for this study, with only 14 pregnant women (7 low-risk and 7 high-risk) included, so the lack of statistical significance could also be due to insufficient data.
[5] https://www.nature.com/articles/nature05058.pdf?origin=ppub
One Reply to “The matter of maternal mucus: permeability and preterm birth”